
Key Takeaways
- Extreme fatigue in the first trimester is biologically normal — progesterone is doing that
- The second trimester often brings better sleep, but heartburn and leg cramps can start creeping in
- Third trimester is the hardest: position restrictions, bathroom trips, restless legs, and anxiety all converge
- Left-side sleeping is recommended after 20 weeks for circulation, but don't panic if you wake up on your back
- Magnesium glycinate and melatonin (low dose) are generally considered safe, but always check with your OB first
- Restless Legs Syndrome (RLS) affects up to 26% of pregnant women — it's treatable, not just something to endure
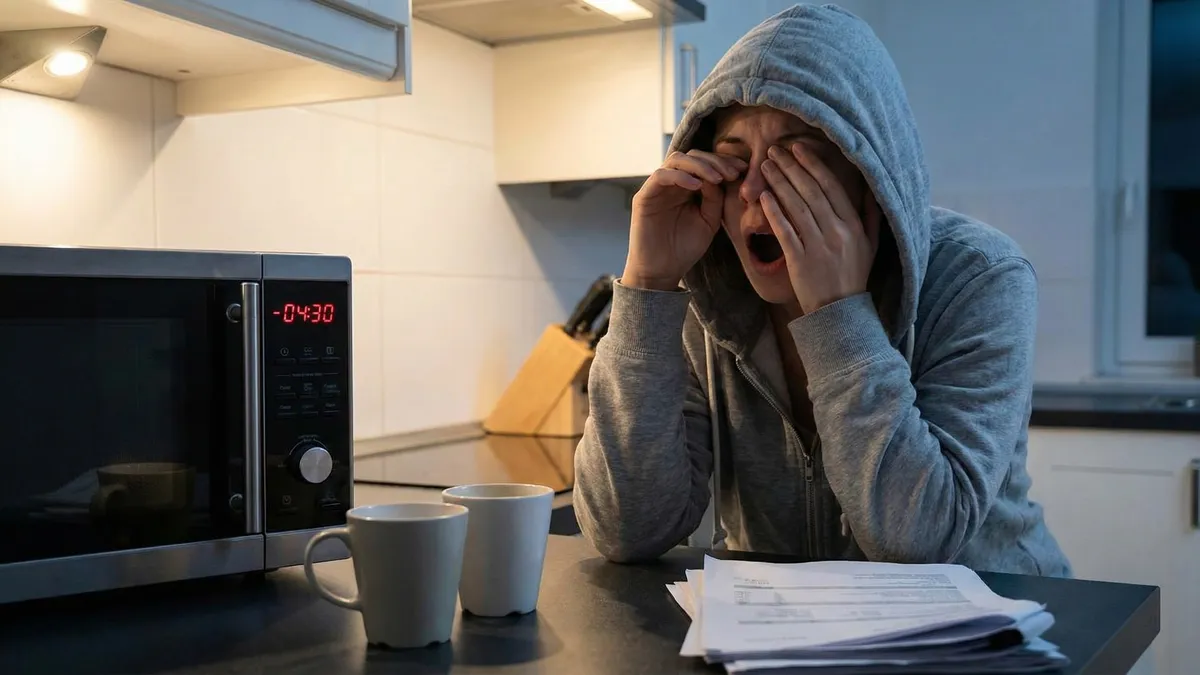
Nobody tells you the full truth about pregnancy sleep. "You'll be tired" doesn't begin to cover it. You'll be cosmically, bone-deep exhausted in ways that feel almost medical — and in the first trimester, they basically are. Then around the second trimester you'll get a window of relief that lulls you into thinking you've figured it out. And then the third trimester arrives and your body becomes an obstacle course between you and a full night's rest.
I haven't been pregnant, but I've spent enough time in sleep research and talking to people who have been to know that the generic advice ("sleep on your left side! avoid caffeine!") misses about 90% of what's actually hard about this. So let's go trimester by trimester, be specific about what's happening and why, and talk about what actually helps.
01 First Trimester: The Exhaustion Nobody Warned You About
Weeks 1–12 are, for many people, the most surprising sleep period of the entire pregnancy. Not because sleep is bad, exactly — it's that you need so much more of it and still wake up feeling like you've been hit by something. You may be sleeping 10, 11, 12 hours and still dragging yourself through afternoons. This is not weakness. This is progesterone.
Progesterone Surge
Progesterone — which skyrockets in early pregnancy — is a natural sedative. It promotes NREM sleep, which sounds good, but it also fragments sleep architecture and can cause you to feel drowsy even after a full night's rest.
Frequent Urination Starts Early
Blood volume increases by up to 50% during pregnancy, and your kidneys process it faster. Most people start waking once or twice a night to urinate by weeks 6–8 — well before the baby is big enough to physically press on the bladder.
Nausea Doesn't Keep Office Hours
"Morning sickness" is a cruel misnomer. For roughly 80% of people with pregnancy nausea, it hits at night too — sometimes worse, because there's nothing in the stomach and you're lying still. This is one of the least-discussed sleep disruptors of early pregnancy.
Anxiety and Hyper-Alertness
The brain becomes acutely attuned to the pregnancy in the first trimester, especially if there's been a previous loss or fertility treatment. This shows up as racing thoughts at bedtime, difficulty getting back to sleep after waking, and light sleep overall.
Nap Without Guilt
A 20–30 minute nap in the early afternoon is genuinely restorative and won't significantly disrupt nighttime sleep. Your body is doing extraordinary metabolic work right now. Rest is not laziness.
Small Snacks for Nausea
Keep plain crackers or dry cereal on the nightstand. Eating a few crackers before lying down — and if you wake up nauseous at night — can significantly reduce nausea-driven disruptions. An empty stomach makes nausea worse.
Hydrate Earlier, Not Later
Front-load your fluid intake before 6pm and taper off in the evening. You'll still wake up to urinate, but doing this can reduce the number of trips from 3–4 down to 1–2.
Don't Fight the Fatigue
If you need to sleep at 8pm, sleep at 8pm. Your social calendar and sense of self can survive this phase. Pushing through first-trimester fatigue doesn't make you tougher — it just makes you more depleted.
02 Second Trimester: The Brief Golden Period (and Its Ambushes)
Weeks 13–26 are, for many pregnant people, a significant improvement. Progesterone levels stabilize. Nausea typically fades. The baby isn't yet big enough to create serious physical discomfort. Sleep quality genuinely improves for a lot of people during this window, and if you're in that camp — enjoy it without guilt.
But the second trimester is also when several new disruptions start introducing themselves, often quietly at first:
Vivid Dreams Intensify
Hormonal shifts and increased REM activity lead to extraordinarily vivid, sometimes disturbing dreams. This is normal. It doesn't mean anything is wrong — your brain is just running hot.
Heartburn Begins
Progesterone relaxes the lower esophageal sphincter, and as the uterus grows, it begins putting upward pressure on the stomach. Lying flat makes reflux worse — this is when elevation strategies and meal timing start to matter.
Back Pain and Hip Discomfort
The center of gravity is shifting. Ligaments are loosening due to relaxin. Back and hip pain during sleep starts appearing, especially for side sleepers who don't yet have the right pillow setup.
Leg Cramps
Nocturnal leg cramps — sudden, painful calf spasms — are common throughout pregnancy but often start in the second trimester. They're linked to mineral deficiencies (particularly magnesium and calcium) and can be genuinely severe enough to wake you from deep sleep.
Heartburn at Night: What Actually Helps
• Stop eating 2–3 hours before bed
• Elevate the head of your bed (a wedge pillow works better than extra pillows, which can strain the neck)
• Avoid acidic foods, chocolate, citrus, and carbonated drinks in the evening
• Sleep on your left side — this positioning reduces reflux compared to the right side
• Talk to your OB about safe antacids: calcium carbonate (Tums) is generally approved, but check before taking anything
03 Third Trimester: Where Sleep Goes to Be Complicated
Weeks 27–40 are widely reported as the hardest for sleep — and with good reason. By this point you're dealing with a combination of physical discomfort, biochemical disruption, and what your body seems to interpret as a pre-birth preparation mode. Multiple things conspire against you at once:
Physical Challenges
- Can't find a comfortable position
- Bathroom trips every 2–3 hours
- Baby movement (sometimes vigorous) at night
- Shortness of breath when lying down
- Hip and back pain from weight and posture
Neurological Challenges
- Restless Legs Syndrome (RLS)
- Anxiety and anticipatory wakefulness
- Racing thoughts about birth and newborn care
- Sleep apnea risk increases significantly
- Reduced melatonin efficiency
Restless Legs Syndrome in Pregnancy
RLS deserves special attention because it's both common and genuinely underdiagnosed. Studies estimate it affects 10–26% of pregnant women, with rates increasing in the third trimester[1]. The sensation — an overwhelming urge to move the legs, worse at rest, temporarily relieved by movement — is not just "uncomfortable." It can make sleep effectively impossible on bad nights.
The connection to pregnancy is likely related to iron deficiency (ferritin levels fall as blood volume expands) and folate status. Before assuming RLS is just something to endure, ask your OB to check your ferritin level. Iron supplementation — if levels are genuinely low — can dramatically reduce or eliminate RLS symptoms in pregnancy[2].
Sleep Apnea Risk Is Higher Than Most People Realize
Pregnancy significantly increases sleep apnea risk due to weight gain, nasal congestion from increased blood volume, and airway changes. Untreated sleep apnea in pregnancy is associated with gestational hypertension, preeclampsia, and gestational diabetes. If your partner reports loud snoring, or you wake with headaches and feel unrested despite adequate time in bed — bring this up with your OB. It's not just snoring. It's worth investigating.
04 Sleep Positions: The Left-Side Guidance and What It Actually Means
You've probably heard "sleep on your left side" and possibly been terrified every time you woke up on your back in the third trimester. Let's clear this up, because the anxiety itself disrupts sleep.
Why Left Side?
Left-side sleeping keeps the uterus off the inferior vena cava (the large vein running along the right side of your spine), improving blood return to the heart and circulation to the placenta. It also reduces pressure on the liver and can help with heartburn.
Don't Panic About Back-Sleeping
Large studies have not found that occasional back-sleeping causes harm[3]. If you wake up on your back, simply roll to your side. The anxiety of trying to stay on your left all night can be more disruptive than the position itself.
Pillow Strategy
A full-length body pillow (or a dedicated pregnancy pillow) changes everything in the third trimester. Support goes between the knees to align the hips, behind the back to prevent rolling, and under the belly to take pressure off the uterine ligaments.
Right Side Is Also Fine
Right-side sleeping is not dangerous. The left-side preference is about optimization, not about avoiding harm. If your left hip aches and your right side feels better — use your right side.
"Discomfort is a signal. It will wake you up. Trust that your body will not let you stay in a position that's dangerous without telling you."
— Common reassurance from maternal-fetal medicine specialists, echoed in clinical guidance
Pillow Configurations That Actually Work
Generic advice says "use a pregnancy pillow." Here's what more specific pillow use looks like in the third trimester:
Between-Knees Support
Stacking the hips without a pillow between the knees creates significant joint torque. A firm pillow between the knees (thicker than you'd use normally) keeps the pelvis neutral and reduces hip and lower back pain.
Belly Support
A softer pillow or rolled towel tucked under the belly when lying on your side reduces the pull on the round ligaments — which is what causes that sharp, often alarming pain people feel in pregnancy when rolling or changing position.
Back Blocker
If you're worried about rolling to your back, placing a firm pillow or foam wedge against your back creates a physical barrier. Some people use a tennis ball sewn into the back of a shirt — uncomfortable enough to wake you but not to hurt you.
Head Elevation for Reflux
A wedge pillow under your upper body (not just extra pillows under the head) genuinely reduces nighttime reflux. The incline needs to be gradual and support the full torso — propping just the head can actually worsen reflux by bending the body at the waist.
05 Supplements and What's Actually Safe
This is the section where I have to be most careful, because pregnancy pharmacology is genuinely nuanced and "generally considered safe" is not the same as "safe for your specific situation." Always loop in your OB or midwife before starting anything. That said, here's what the evidence looks like for commonly discussed sleep supplements during pregnancy:
Magnesium Glycinate
Generally well-supported for pregnancy. Magnesium helps with muscle relaxation (including leg cramps), sleep quality, and may reduce RLS symptoms. Glycinate form is better tolerated than oxide or citrate. Typical dose is 200–400mg before bed. Check with your provider — magnesium is often already in prenatal vitamins.
Melatonin (Low Dose)
Limited but generally reassuring data for short-term use at low doses (0.5–1mg). Useful for jet lag or shift work disruptions. Not well-studied for long-term use in pregnancy. Not a first-line recommendation. Check with your OB before using, even occasionally.
Things to Avoid
Valerian root: insufficient safety data in pregnancy. Diphenhydramine (Benadryl/ZzzQuil): widely used but some concerns about neural tube effects in first trimester. Herbal teas beyond confirmed-safe varieties: chamomile is generally okay, but many herbs are not studied. When in doubt, skip it.
Iron and RLS
If you're experiencing restless legs, ask your provider to check your ferritin specifically (not just hemoglobin). Ferritin can be low even when hemoglobin looks normal. Low ferritin is strongly associated with RLS, and supplementation — if appropriate — often helps significantly within a few weeks.
06 When to Call Your Doctor
Most pregnancy sleep disruption is normal and manageable without medical intervention. But some things warrant a call — not because they're necessarily dangerous, but because they're treatable and you don't have to just suffer through them:
Contact Your Provider If You Experience:
• Loud snoring with apnea episodes (breathing pauses reported by a partner) — sleep apnea in pregnancy needs evaluation
• Severe insomnia lasting more than 2–3 weeks that isn't responding to any behavioral changes — cognitive behavioral therapy for insomnia (CBT-I) is safe in pregnancy
• Restless legs so severe they prevent sleep most nights — ferritin testing and possible iron supplementation can help
• Severe heartburn that isn't responding to elevation and dietary changes — there are pregnancy-safe medications
• Any sleep disruption that feels disproportionate or is affecting your ability to function during the day — you don't have to normalize everything
One specific flag: if you're in the third trimester and you notice you're sleeping much better than expected — sleeping deeply and not waking — and you're also noticing reduced fetal movement, call your provider. This combination can occasionally indicate a problem worth checking.
07 A Brief Word About What Comes Next
I'd be doing you a disservice not to mention that postpartum sleep is its own entirely separate chapter, and probably a harder one for most people than pregnancy sleep. Newborn sleep is non-negotiable in its demands on your schedule — they wake every 2–3 hours, they don't distinguish night from day for several weeks, and feeding (whether breast or bottle) happens on their timeline, not yours.
A few things that are genuinely useful to know in advance:
"Sleep When the Baby Sleeps" is Partially True
It's not always possible — sometimes you eat, sometimes you shower, sometimes you just sit in silence and stare at the wall. But if you can get even one 90-minute block during the day when the baby naps, it matters. Prioritize sleep over housework whenever you can.
The Partner Dynamic Matters
If you have a partner, explicit conversations about who handles which nighttime shifts — ideally before the baby arrives — reduce conflict and ensure that both of you are getting some continuous sleep. Continuous sleep is more restorative than the same amount of fragmented sleep.
Postpartum Insomnia Is Real
Some new parents develop hyperarousal — lying awake even when the baby is sleeping, unable to stop monitoring for sounds, stuck in high-alert mode. If this persists past a few weeks, it's worth mentioning to your provider. It's treatable, and it's not just "new parent nerves."
It Does Get Better
Most babies establish longer sleep stretches by 3–6 months. The newborn phase is genuinely hard — one of the hardest things sleep-wise that most people ever experience — but it is temporary. That's worth remembering at 3am.
The honest summary
Pregnancy sleep is a moving target. What disrupts your sleep in week 8 is completely different from what disrupts it in week 32 — and the solutions are different too. The one through-line across all three trimesters is this: your body is doing something extraordinary, and what it needs (more rest, different positions, specific nutrients) is not irrational or excessive. It's metabolic reality.
Work with the biology rather than fighting it. Nap in the first trimester. Adjust positions and pillows as you grow. Address specific symptoms — RLS, heartburn, leg cramps — specifically rather than just tolerating them. And keep your provider in the loop about anything that's genuinely disrupting your function, because there's usually more that can be done than you might think.
You're not just "tired because you're pregnant." You're running a construction project at the cellular level, around the clock, for nine months. Sleep is the maintenance window. Protect it as best you can.
Sources & Further Reading
- "Restless legs syndrome: prevalence and impact in women — a study in five European countries." Journal of Clinical Sleep Medicine, 6(6), 548-554. (2010) PubMed →
- "Restless legs syndrome and sleep disturbance during pregnancy: the role of folate and iron." Journal of Women's Health & Gender-Based Medicine, 10(4), 335-341. (2001) PubMed →
- "Stillbirth risk associated with maternal sleep position in late pregnancy: a prospective nationwide study." EClinicalMedicine, 10, 49–57. (2019) PubMed →